.jpg "a flutter with rvr treatment")
The rest of the pharmacological agents used as antiarrhythmics fall under the fifth class with different mechanisms of action from the previous classes. There are four specific classes of antiarrhythmics with specific physiological functions divided into classes based on their mechanism of action. Vaughan-Williams Anti-arrhythmic Classification This Calcium Channel antagonism leads to decreased SAN chronotropic effect and decreased AVN conduction, making it useful for treatment of atrial arrhythmias such as AF, Atrial Flutter and Supra-ventricular Tachycardias (SVTs).Non-dihydropyridine CCBs are more selective to L-Type Calcium Channels in cardiac cells, such as the Sino Atrial Node (SAN) and Atrio Ventricular Node (AVN), although all CCBs cause peripheral vasodilation.Can be further divided into benzothiazepines (not to be confused with benzodiazepines) and phenylalkylamines.These CCBs are those which generic name does not end with “pine”. 
Their hemodynamic effects can be associated with adverse effects such as hypotension and reflex tachycardia secondary to sympathetic stimulation as a compensatory mechanism for the decreased cardiac output.Because of this peripheral calcium channel selectivity, they are commonly used for treatment of Hypertension and angina.DHP CCBs are more selective to peripheral vasculature than cardiac cells, leading to arterial smooth muscle relaxation and decreased Systemic Vascular Resistance (SVR), thus, decreasing afterload and Myocardial Oxygen Demand (MVO2).These CCBs can be easily identified by the last four letters of the generic name ending with “pine”.These particular pharmacological agents can be further divided into subdivisions based on their molecular composition: The patient was now asymptomatic and admitted for observation without further incident.ĭiltiazem (Cardizem) is a Class IV antiarrhythmic and one of the most common pharmacological agents used for treatment of AF with RVR.Ĭlass IV antiarrhythmics are Calcium Channel Blockers (CCBs), which inhibit intracellular calcium influx via calcium channel antagonism. There are no signs of subendocardial ischemia, suggesting the ST-segment depression was rate-related. Procainamide is another lesser used choice after rate is controlled.There is a sinus rhythm with left ventricular hypertrophy by limb lead voltage criteria and left atrial enlargement. Amiodarone (150 mg IV loading dose infused over 10 minutes, followed by 1 mg/min infusion for 6 hours, a 0.5-mg/min infusion for 18 hours, and then a reduced IV dose or oral dose) is also effective in converting atrial flutter to normal sinus ryhthm. It may be repeated once, but the provider should be aware it has a potential risk of inducing torsades de pointes, so the patient needs to be monitored carefully for 4-8 hours after drug administration. Ibutilide, a class III antiarrhythmic (Corvert, 1 mg in 10 mL saline infused slowly over 10 minutes) is effective in converting new-onset atrial flutter patients to normal sinus rhythm 90% of the time. 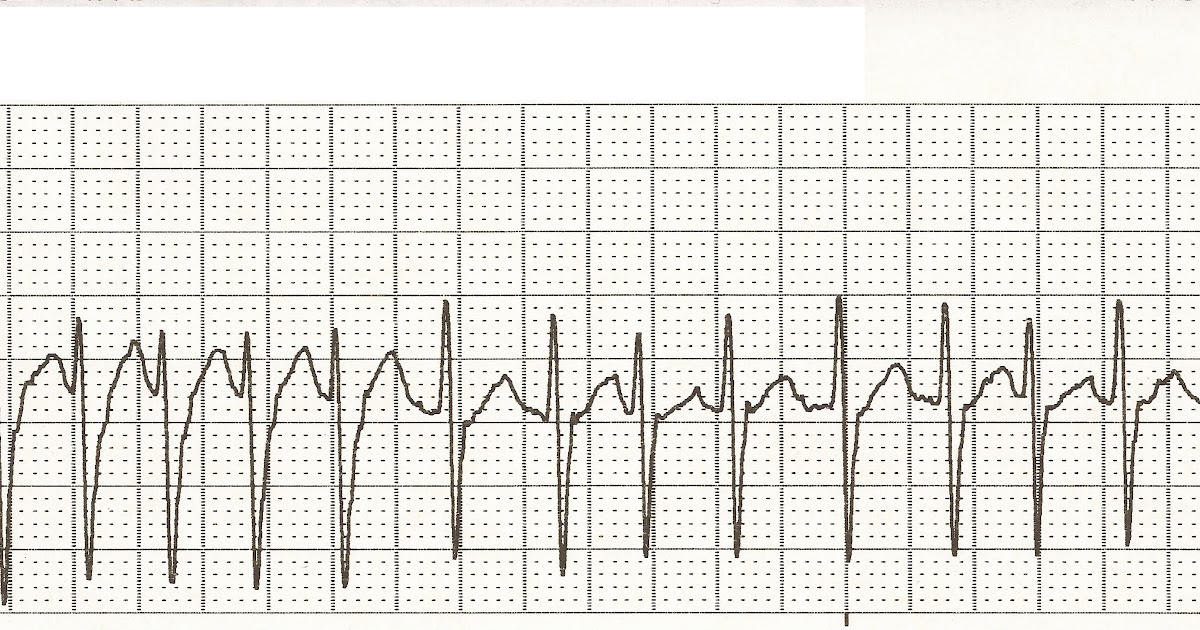.jpg "a flutter with rvr treatment")
If synchronized DC cardioversion is utilized in a non-emergent setting, the provider must be certain that the atrial flutter is new-onset, that a patient does not have thrombosis in the heart via echo, or that the patient has been adequately anticoagulated in order to prevent a thromboembolic event. If a patient is hemodynamically unstable and/or has an excessively rapid ventricular rate you may consider an antiarrhthmic drug or synchronized DC cardioversion. Beta blockers and CCB are effective in prophylactic prevention of atrial flutter after postoperative thoracic or cardiac surgery. Drugs of choice include beta blockers such as esmolol (0.5 mg/kg IV bolus followed by 50-300 ucg/kg/min) and propranolol, or calcium channel blockers such as verapamil (5-10 mg IV) or diltiazem. Initial treatment of atrial flutter targets the rate control (which is frequently ~150 BPM).
0 Comments
Leave a Reply. |
AuthorWrite something about yourself. No need to be fancy, just an overview. ArchivesCategories |
 RSS Feed
RSS Feed
